 |
| Adhisthana, June 2018 |
After the AGM, the presentations started with someone from Diabetes UK updating us on what they've been up to in the way of nutritional news. This included information and new videos about 'Diabulimia', which is a term often used (but just as often criticised) describing the practice of someone with Type 1 Diabetes withholding insulin in order to lose weight.
Then a doctor ran through all the current technologies available at the moment, including insulin pumps, CGM systems, Flash GM systems, sensor-augmented pumps, closed loop and artificial pancreas systems, and something called Diaport which delivers insulin into the peritoneal cavity. There wasn't really anything new here for me, but it was nice to appreciate that my knowledge is way ahead of many Dietitians who don't come into contact with these technologies in their usual work setting.
Quite a few Diabetes Dietitians are working at national policy level with Diabetes UK and the All Party Parliamentary Group on Diabetes. This year the old evidence-based nutrition guidelines from 2011 were updated with a new document, which has shifted away from nutrients (recommended proportions of protein, fat and carbohydrate in the diet) in favour of real foods. The overarching recommendations haven't changed: the first line treatment of Type 2 Diabetes should be weight loss of 5%, a Mediterranean style of eating, education and exercise. For Type 1 Diabetes it is still about matching insulin to carbohydrate intake to regulate blood glucose levels. The advice about prevention of cardiovascular disease is now aligned with the NICE guideline, and progress has been made on the thorny question of fat - is it in fact irrelevant, or should we still advise restriction? The conclusion is now that the quantity of fat is less important than the type of fat, and whatever level of fat we choose to eat it should be more unsaturated than saturated.
The 'James Lind Alliance Research Priorities' were also new to me - the ten highest priority research topics in various clinical areas, including diabetes. Not that it makes any difference to my workload, but interesting to see what questions are thought to be most important at this time. A couple of the priorities relate to diet, and one is the old chestnut about the role of fat, protein and carbohydrate in the diet for Type 2 Diabetes, and what the evidence tells us we should specifically be advising people to eat. This has been addressed by the finest minds in the UK Dietetic profession, and the answer is that we have no idea. Another question that still remains unanswered is what we would initially advise someone with Type 2 Diabetes who is not overweight.
Those same fine minds have also come up with a policy statement about low carbohydrate diets (defined as between 50g and 130g carbohydrate per day) in the management of Type 2 Diabetes. It was published in the week following the study day, and it's handy to be able to see a summary of the available evidence even if that evidence is scanty. Essentially, we can say that in the time frame of 12 months, adopting a low carbohydrate diet is as good as any other approach to improving blood glucose levels, and it probably works because restricting carb tends to result in a reduction in total energy intake and therefore weight loss. We don't have any evidence beyond 12 months because it seems to be quite a difficult diet to sustain.
The next presentation was all about trying to be more prescriptive about how to manage exercise with Type 1 diabetes. I have written about this before (June 2016), and said at that time that it's one of the most difficult aspects of diabetes. A Dietitian from Birmingham Children's Hospital has worked on this for a while, and come up with a spreadsheet that allows you to enter six parameters: what kind of exercise; what intensity; the duration; how long since your last insulin bolus; whether you want to reduce your insulin or increase your carb intake; and whether you use an insulin pen or a pump. It then comes up with its best guess (based on published evidence) on how to manage blood glucose, food and insulin before, during and after the activity. You can print that recommendation for the patient to try, but it may need adjusting subsequently.
The most interesting presentation was from a Dietitian involved with the DiRECT trial, which has attracted the largest amount of research funding that Diabetes UK has ever awarded. The trial is intended to follow up an earlier 'Proof of Concept' trial that suggested that Type 2 Diabetes could be reversed with rapid weight loss, and this time they want to try and find out how it works, how much weight loss is needed, how long does reversal last, who might benefit the most from this approach and whether it can be achieved in primary care. Weight loss is achieved through Total Diet Replacement for 12 to 20 weeks (the Cambridge Weight Plan meal replacement products) with weekly or fortnightly review, followed by structured food reintroduction with fortnightly review, and there is also support in increasing physical activity. Monthly monitoring and support is provided to stabilise weight and prevent weight regain for two years.
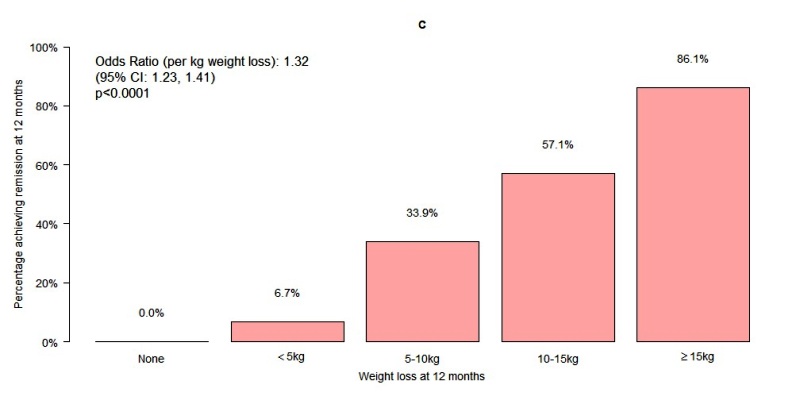
There were relatively few participants (n=157) and the trial is not yet finished, but early results are impressive. Of the cohort who managed to lose 15kg or more, irrespective of their starting weight, 86% achieved remission from their diabetes at 12 months, defined as normalised blood glucose results (there are ongoing discussions about the definition of remission). Results were better for younger participants, lower starting HbA1c results and when the duration of diabetes was shorter. Unfortunately this exactly defines the people I don't see - in secondary care we generally see people who have had Type 2 Diabetes for some time and whose medication regimes are escalating and/or who are starting to get complications.
The last presentation of the day was from the doctor who leads the Diabetes service at the hospital we visited over the summer, talking about interpreting the data that we are starting to see coming from all these technological wonder-gadgets. One key point: we often advise a minimum of 4 blood glucose tests a day, but the evidence suggests this can generally only get people down to an HbA1c of about 69mmol/mol (8.5%). The target is often 53mmol/mol (7%) which would take at least 8 fingerprick tests a day, and for anything lower than this you're looking at micro-management using a CGM and pump or artificial pancreas system.
It was an interesting and informative day, but I continue to remind myself that despite the worth of the ideas being presented, there is in reality a negligible chance of making any changes to the service we offer, given that nothing has changed even after the whole team's visit to London.

As usual, a very interesting blog, exposing the human gap between research and application. Did I hear four days ago that NHS England suggests that disposable insulin needles and test strips should not be provided on prescription because "there were cheaper or better alternatives"? If so, and if I didn't mishear, what alternatives?
ReplyDeleteSome time ago (October 2013) you mentioned islet transplantation, whereby isolated human islets were whizzed up and introduced into some byway of the body to lodge and implant in the liver. Has there been progress with this?
I have heard that blood glucose meters are being swapped for meters with cheaper strips, and that there is a plan to encourage prescription of cheaper needles. I have no more information about islet transplants!
DeleteI forgot: https://www.england.nhs.uk/wp-content/uploads/2018/11/06i-pb-28-11-2018-lpp-gff-annex-a-items-not-routinely-prescribed-update.pdf It is only a consultation document, marked OFFICIAL-SENSITIVE-COMMERCIAL and in
ReplyDeleteinstantly leaked to the Press.